Ep. 2: Week 2 Baby w/ Dr. Lisa Durette – Developing Mighty Minds

Tyrant Farms' articles are created by real people with real experience. Our articles are free and supported by readers like you, which is why there are ads on our site. Please consider buying (or gifting) our books about raising ducks and raising geese. Also, when you buy through links on our site, we may earn an affiliate commission. Learn more
Episode 2: Developing Mighty Minds’ WEEK 2 BABY interview with child and adolescent psychiatrist, Dr. Lisa Durette, and parents Susan (aka The Tyrant) and Aaron von Frank.
Main topics discussed in this episode:
- Adjustment into the world of parenting (from the parents’ perspective): how did expectations match reality?
- Co-sleeping and bedsharing with baby: pros, cons, and best practices.
- Best way to talk to your baby for brain development: goo-goo-ga-ga or speaking to them like little adults?
- When do you introduce baby sign language?
- How (and how quickly) should a parent/primary caregiver respond to the cries of an infant?
- Are there any mental health benefits for mom and baby that arise through the act of breastfeeding (beyond nutrition)?
Watch the Week 2 Baby video interview:
*Note: video may not display or play if you run ad blocking software. Please temporarily disable ad blocking software to view video. Ads help us pay to create this website, so thanks for your support!
Read the Week 2 Baby discussion:
Prefer to read rather than watch the video? Or want to follow up on something you heard?
Here are highlights from the Week 2 Baby discussion with parents Aaron and Susan von Frank and child & adolescent psychiatrist, Dr. Lisa Durette:
1. Question: From Lisa to parents (Susan and Aaron): What has the adjustment been like into the world of parenting? What rhythms has Week 2 Baby started to get into, if any?
From the parents:
Three big challenges during transition to new parenting that we were expecting:
- dirty diapers,
- all the extra chores and work associated with having a baby to care for,
- lack of sleep.
How our expectations matched reality:
Baby diapers have not been overwhelming for us because we’ve had pet ducks for many years, which wear diapers when we bring them indoors. Having diapered ducks prepared us for gross human baby diapers!
Having two parents/primary caregivers at home has really helped reduce the stress of transition to parenting a human baby. If it’s possible for the second caregiver/parent to be at home during this transitional period, we highly recommend doing so.
We have the deepest respect (and sympathy) for single parents. If you’re a single parent, get help from your network (family, friends, etc) to help during the adjustment – meals, cleaning, baby care while you nap, etc. Your mental health and wellbeing isn’t just important for you, it’s also important for your baby’s mental health.
Co-sleeping and bedsharing with baby
[Definitions for clarity: Co-sleeping means sleeping near your baby, e.g. in the same room, but not necessarily in the same bed. Bedsharing means sleeping in the same bed with your baby.]
We’re new parents, and we’ve been getting sleep! How are we reasonably well-rested at Week 2 in baby’s life?
We’ve been practicing safe co-sleeping and bedsharing with our baby, following guidance from La Leche League International. (*See: LLLI’s Safe Sleep 7 and Bedshare guides, plus consider reading the book: The Womanly Art of Breastfeeding).
Co-sleeping (including bedsharing) is what virtually every culture around the world has done throughout human history, but it may create an elevated risk of SIDS (sudden infant death syndrome) under certain circumstances and/or if precautions aren’t taken.
What about the elevated risk of SIDS and recommendations by most US medical organizations NOT to bedshare with your baby due to elevated SIDS risk? Here’s why we’re comfortable with the risk:
- our baby is healthy and full-term;
- we’re not smoking or drinking alcohol;
- we’re breastfeeding;
- we’re following all of the co-sleeping safety recommendations; and
- we’re using an Owlet Smart Sock device which monitors our baby’s vitals and alerts us (loudly) the second there’s a problem.
In other words, the already low risk of SIDS is virtually non-existent in our specific circumstances. However, there’s a big benefit of bedsharing for our family: we’re able to get plenty of quality sleep together. This improves our mood and mental health, making parenting easier. Bedsharing isn’t for everybody; it should only be done if parent(s) and baby both fall into low-risk categories AND necessary precautions are taken.
According to Centers for Disease Control (CDC), there were a total of 1,300 SIDs deaths in the most recent year for which data is available (the vast majority of these deaths are unrelated to bedsharing). SIDS rates are higher in the southeast US where we live, perhaps due to higher temperatures and socio-economic factors.
Bottom line: our adjustment to new parenthood has been way better than we expected, thanks largely to our ability to get sleep! Our ability to get sleep has been due to practicing safe bedsharing with our newborn. Just to reiterate: bedsharing should only be done by people in low-risk categories who follow all necessary safety precautions so as to reduce SIDS risk.
Side note: Our newborn had jaundice early on, a condition caused by high bilirubin levels. Jaundice affects up to 60% of full-term newborns. It takes a couple weeks for breastfed babies to overcome jaundice. How did our pediatrician know our newborn was no longer at risk of jaundice? Blood testing to monitor bilirubin levels, plus baby stopped losing weight and started having yellow poops as mom’s milk came in, allowing baby to excrete bilirubin.
2. Question: What’s the best way to talk to your baby to stimulate their mighty minds? Ga-ga-goo-goo or speaking to them like little adults?
You can’t really make a double-blind placebo controlled study (gold standard) to give a definitive answer on this question. However, what we can say is this: there’s plenty of research showing the more baby is exposed to language early on, the better they do at their own language development. Ga-ga-goo-goo isn’t actually language, it’s sounds that don’t convey actual meaning.
Recommendation: speak to your baby in your natural language and in your natural voice. No, a voice on TV or radio or voices of non-primary caregivers aren’t a sufficient replacement for the voice(s) and language of baby’s primary caregiver(s). That’s who and what they tune into and need to hear for their own optimal language development.
Can baby recognize repeated songs or words?
Yes! The more baby hears something repetitively from their primary caregiver(s), the more it strengthens and utilizes the neuronal connections in their brain. The whole “use it or lose it” notion of baby brain development discussed during Week 1.
Interesting side note: later on, a 1- or 2-year-old who can’t actually read a book will still know if you’ve skipped a page in their favorite story book because they’ve heard it enough times to recognize it and know something is missing. That’s pattern recognition due to repetition from their primary caregiver, so don’t think you can get away with making your story time a little shorter — your child will likely call you out on it!
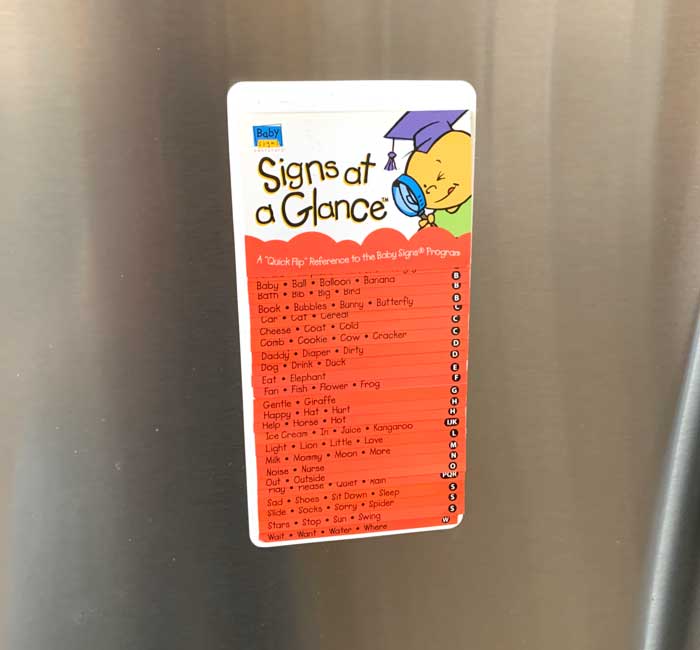
What about baby sign language? When should you introduce sign language to your baby?
Baby sign language reduces baby frustration because it allows them to express their needs to their primary caregiver(s) before they’re able to use spoken language. Parents who plan to do so, should pick the 5-10 most common signs (hungry, thirsty, diaper change, etc) and start using them around month 4, even though baby won’t be able to start signing until much later down the road.
3. Question: How (and how quickly) should a parent/primary caregiver respond to the cries of an infant? Our understanding is that in the first few months after birth, infants need to feel like their calls for action (or milk) are being heard and met almost immediately in order to feel confident that their needs will be met. Is this accurate or is there more to it than that?
It’s important to recognize that a newborn baby is 100% dependent on its parents for all of its needs. Your responsiveness to your baby’s needs and cries for help are critical for the formation of trust between parent and baby.
Example: Children raised in large orphanages who’s needs aren’t being met when they cry and/or who don’t have primary attachment figures have been shown to have much higher risks of attachment disorders that lead to difficult psychopathologies later in life (source). This is obviously an extreme example, but NOT responding to your newborn’s needs can actually have negative lifelong impacts.
There isn’t a set time period for when you should respond to your baby’s cries, but it’s best that you respond as soon as you’re able to.

4. Question: Are there any mental health benefits for mom and baby that arise through the ACT of breastfeeding? (Not talking about the benefits of breastmilk itself, just the process of breastfeeding.)
The process of breastfeeding assists with the formation of bonding and attachment. But so can bottle feeding, so if you choose to bottle feed or have to bottle feed, don’t feel guilty!
*Baby is starting to have a meltdown at this point, so we have to wrap up the conversation ASAP. More on this topic in future episodes!
More in Developing Mighty Minds:
- Introduction to Developing Mighty Minds
- Ep. 1: Week 1 newborn baby
- Week 3 Baby (coming soon!)
Subscribe to Tyrant Farm’s Parenting (below) to get the latest Developing Mighty Minds episodes as they’re published!





